Healthy Aging: Oxymoron or Opportunity? Part 3
In “Healthy Aging,” Parts I and II (Flourish, Fall 2025 and Winter 2026), we explored the impact of aging on our muscular, skeletal, cardiovascular, digestive, endocrine, and immune systems and our metabolism. We also looked at how getting older affects cognition, a major function of the central nervous system.
In this edition, we’ll delve into the effects of getting old on our peripheral nervous system, and the special senses that are our link to the world around us.
Let’s face it: unless you’re under the age of about 50, you probably don’t see, hear, smell, or taste as well as you used to. While the impact of aging on vision and hearing gets a lot of press, I’d like to begin with our sense of smell. This is in part because it’s considered to be the oldest of our senses, but also because it’s the one sense that, quite literally, eludes me.
You see, as a kid, I was certain that smell was something my brothers made up to torment me (a psychologist would have a field day with that one, I know). To get at the truth, I regularly took each of my siblings aside and asked them to describe for me what something smelled like. Their answers were remarkably alike. That’s when I came to understand that sense of smell was a real thing! And apparently, I didn’t have one, a condition I later learned is called anosmia.

Smell
It was long thought humans could detect 10,000 different scents, but in fact, the average person—excluding us anosmics—can distinguish at least a trillion scents (1,000,000,000,000). We detect them by inhaling air that contains odour molecules that then bind to receptors in the nose, which send messages to the brain. This important process allows us to find food, stay safe, and helps us to establish and maintain social relationships and emotional bonding.
This is why a significant reduction in smell can have big implications for more than 50% of people aged 65 and older who experience it. Those with loss of smell are not only more likely to develop anxiety and depression: they’re also less able to identify dangerous odours including noxious chemicals, leaking gas, smoke, and spoiled food.
Age-related loss of smell, known as presbyosmia, appears to result from several factors, including gradual decline of olfactory receptor neurons, changes in the nasal lining, alterations in mucus that helps transport odour molecules, and reduced neural processing of smell signals in the brain. What’s certain is that some medications—including antibiotics; cholesterol-lowering drugs; and heart, thyroid, and blood-pressure medications—can also dampen this valuable sense.
So, how can you lend your nose a hand? Talk to your health-care practitioner about your medications; if you smoke, do your best to quit; and protect yourself at home by buying smoke and gas detectors and applying the “when in doubt, throw it out” rule of cleaning out the refrigerator.
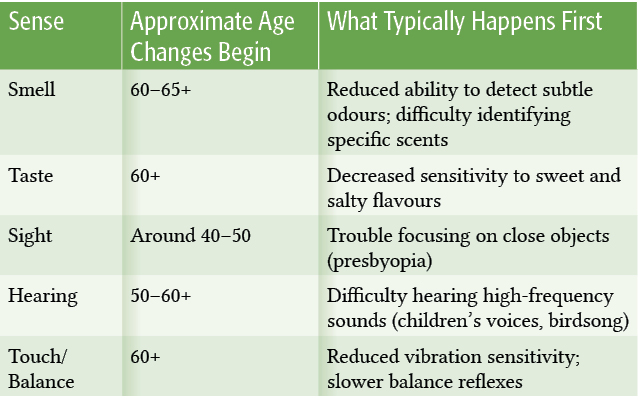
When Do Our Senses Begin to Change?
Aging doesn’t switch off our senses overnight. Most begin to shift gradually—often decades before we notice.
Taste
Adults have roughly 10,000 taste buds, most of them on the tongue. Each tiny bump is home to specialized cells that help detect the various flavours in the foods we eat—sweet, sour, salty, bitter, and savoury, which is sometimes called umami. Much of what we think of as taste is actually smell, so it’s no surprise that, like our sense of smell, our sense of taste also takes a beating as we age. Over time, taste sensitivity may decline as taste receptor cells renew more slowly, saliva production decreases, and nerve signalling becomes less efficient. Plus, many of those same prescription medications that affect our sense of smell also impact taste.
For many seniors, the first tastes to go south are sweet and salty, and the natural inclination is to add more sugar and salt to foods. While that may make foods taste more palatable, it can also contribute to long-term health problems by raising blood sugar, increasing blood pressure, and contributing to weight gain. Instead, add flavour to your food with hot pepper or mustard, onions, garlic, ginger, lemon or lime juices, and fresh herbs.
While a gradual decline of sense of smell and taste is natural as we age, the loss can also be related to deficiencies in some key micronutrients including zinc and vitamin B, which play important roles in nerve and sensory function. These can be found in seafood and fish, meats and poultry, dairy products, beans, and some fortified foods. If you experience a sudden loss of sense of smell or taste, this may occur with viral infections, including COVID‑19; or, in some cases, it may signal an underlying medical or neurological condition. Anyone experiencing abrupt changes should consult a health-care practitioner.

Sight
They say that failing eyesight in old age is nature’s way of protecting you from shock as you pass a mirror. Loss of vision is, in fact, a change to the eye structures. Beginning around the age of 50, most of us will find our eyes focus more slowly, particularly when reading or looking at close objects. This common change, known as presbyopia, occurs mainly because the lens gradually becomes stiffer and less able to adjust its shape for near vision.
By the time we’re 60, our pupils may have decreased to about a third of the size they were in our 20s, and our field of vision shrinks. Our eyes may become cloudier and more tinged with yellow, signalling a breakdown in the lens’ proteins and the onset of cataracts. Floaters, small collagen fibres from the gel that fills the eye, may obscure our field of vision, and dry eye disease, which is common in aging eyes, can cause inflammation and scarring of the cornea if unaddressed.
If all this sounds a bit dark, there is light at the end of the tunnel. Caught early, many serious eye diseases—such as glaucoma, macular degeneration, diabetic retinopathy, and a detached retina—can be effectively treated.
You can also keep minor eye problems at bay by scheduling regular checkups with your optometrist and touching base with your health-care practitioner to ensure your diet contains sufficient vitamins A, C, and E and lutein.

Hearing
Impaired hearing affects more seniors than any other chronic condition. In fact, nearly a third to a half of older adults suffer a hearing loss serious enough to negatively impact their ability to communicate and maintain relationships with others.
The causes of age-related hearing impairment (called presbycusis) can include normal wear and tear on the tiny hairs and nerve cells in the inner ear, a decrease in the elasticity of the eardrum, a history of exposure to loud noises, or a blow to the head or ear. High-frequency sounds—such as children’s voices and bird’s singing—are often the first to disappear. Over time, consonants such as s, z, t, f, and g become harder to distinguish, and words begin to sound muffled. Conversation can become increasingly difficult, particularly when there is background noise.
Untreated hearing loss can force the brain to work harder and ultimately overwhelm the networks normally tasked with thinking and memory. This is called cognitive overload, and it may contribute to overall cognitive decline and a higher chance of developing dementia. Difficulty in hearing and understanding conversations can also result in social isolation, which in turn leads to less sensory stimulation and shrinkage of the sound processing areas of the brain.
While age-related hearing loss is often irreversible, hearing aids have come a long way since the invention of the ear trumpet in the seventeenth century, so consider getting fitted for one. If you suffer from tinnitus, which is often associated with hearing loss and marked by a loud and persistent sound in the ears, talk to your health-care practitioner about how to best manage the condition.

Touch
So, where does touch fit within our sensory journey? Unlike vision or hearing, it’s not confined to a single organ. Specialized nerve endings in the skin, muscles, joints, and connective tissue detect pressure, vibration, temperature, pain, and movement, continuously informing the brain about our environment and body position.
With age, this system becomes less sensitive. The density of skin receptors declines, nerve conduction slows, and circulation to peripheral nerves may decrease. Light touch, temperature changes, and vibration, especially in the feet, can become harder to detect. At the same time, proprioception, our internal sense of body position, grows less precise. Together, these shifts can affect coordination and balance, helping explain why falls become more common in older adulthood.
Touch also plays an important emotional role. Physical contact, like a handshake, a hug, a reassuring hand, activates pathways linked to bonding and stress regulation. Reduced sensory input and social touch may contribute to feelings of isolation. The encouraging news is that this system responds to use. Regular physical activity, balance training, supportive footwear, and meaningful human connection all help maintain sensory awareness and stability. Touch may not grab headlines, but it quietly keeps us grounded—both physically and emotionally.
Our senses may shift with time, but they rarely disappear. They evolve. And so do we. By paying attention, staying proactive, and embracing support where needed, we preserve not just function but also connection. To people, to memories, to the world itself.
Healthy aging isn’t an oxymoron. It’s an invitation to stay curious, adaptable, and fully alive.

Dale Drewery
Dale Drewery is coauthor of BioDiet: The Scientifically Proven, Ketogenic Way to Lose Weight and Improve Your Health. She is an award-winning journalist and writer with a keen interest in science and human health.
biodiet.org
Further Reading
R.L. Doty and V. Kamath. “The influences of age on olfaction: A review.” Frontiers in Psychology 5 (2014): 20.
S.M. Bromley. “Smell and taste disorders: A primary care approach.” American Family Physician 61, no. 2 (2000): 427–436.
M. Mrowicka, J. Mrowicki, E. Kucharska, and I. Majsterek. “Lutein and zeaxanthin and their roles in age-related macular degeneration—Neurodegenerative disease.” Nutrients 14, no. 4 (2022): 827.
G. Livingston, J. Huntley, A. Sommerlad, D. Ames, C. Ballard, S. Banerjee, C. Brayne, et al. “Dementia prevention, intervention, and care: 2020 report of the Lancet Commission.” The Lancet 396, no. 10248 (2020): 413–446.
G. Marchi, F. Busti, A.L. Zidanes, A. Vianello, and D. Girelli. “Cobalamin deficiency in the elderly.” Internal and Emergency Medicine 12, no. 1 (2020): e2020043.
J.W. Miller, D.J. Harvey, L.A. Beckett, R. Green, S.T. Farias, B.R. Reed, J.M. Olichney, D.M. Mungas, and C. DeCarli. “Vitamin D status and rates of cognitive decline in a multiethnic cohort of older adults.” JAMA Neurology 72, no. 11 (2015): 1295–1303.
